Speculum Retractor Problems
The speculum does not fit over dilator.
Open the speculum slightly and lower it over a 10mm dilator.
The speculum does not fit into the incision.
Make sure that:
- skin incision is at least 2.5 cm in length,
- fascial incision is extended beyond the limits of the skin incision,
- adequate finger dissection is performed before speculum insertion.
The speculum’s flared lips get caught on the skin and soft tissues during insertion.
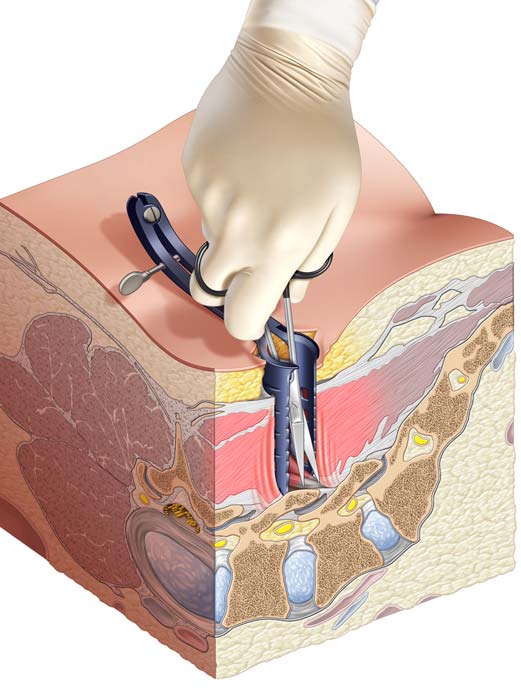
Speculum handle should point cranially or caudally during insertion to help clear skin and soft tissues. When the speculum reaches the depth of the wound, the handle is turned 90 degrees to medial or lateral orientation before the blades are opened.
Muscle (not bone) in visualized at the depth of the wound as the speculum is opened.
This is normal. The speculum is used to expose the musculo-tendinous attachments to the bone. These are then bipolar coagulated, divided with scissors and swept away from the bone.
The speculum does not open far enough cranio-caudally to get pedicle-to-pedicle exposure.
This is normal. Because the speculum blades do not flare, it will not be possible to get a pedicle-to-pedicle exposure with this device through a small incision. That will be achieved later by the Spyder cranio-caudal blades.
Medial-lateral exposure is inadequate with the speculum.
This is normal. The speculum is primarily used to obtain cranio-caudal exposure spanning the facet joint. Additional medial-lateral dissection can be performed after the cranio-caudal Spyder blades have been inserted.
The speculum is unstable in the wound.
This may occur if the patient is too thin.
Solutions:
- Hold the speculum with one hand as you dissect with the other hand.
- In very thin patients, the speculum is not needed, since the facet joint will be quite superficial. Just use a Gelpi to hold the fascia open.
Notes and Bail-Out Strategies